

In order to better understand the current challenges faced by both healthcare providers and the women in their care in Australia and Aotearoa New Zealand, a large-scale data collection and analysis audit is underway as part of a series of sessions taking place at the Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) Annual Scientific Meeting (ASM), held in Wellington, Aotearoa New Zealand in October 2024.
In both these countries, while some hospitals and health care districts collect data on a limited number of labour and birth events and outcomes using the Robson Ten Group Classification System (TGCS)1, this project is aimed at using the Classification System in the collection of many more maternal and neonatal outcomes across both countries in order to analyse trends within healthcare systems by state, rurality, nation and also compare with other data collections which have been made across the world.2

Currently, Australia collects rates of caesarean sections in nulliparous women, via the National Core Maternity Indicators3 and Aotearoa New Zealand collects rates of caesarean sections in Standard Primiparae women via the Maternity Clinical Indicators4, however more detail is needed to understand the trends and patterns in this sphere. It is worth noting that there is a lack of up-to-date, publicly available data via the Maternity Clinical Indicators in Aotearoa New Zealand, which along with the decision not to publish a comprehensive report on the matter since 2012, has made it more difficult to access current and accurate data regarding labour and birth outcomes. Data also has not been made available since 2018 and relies on a web-based tool which further contributes to lack of understanding of birth outcomes in Aotearoa New Zealand.5
The lack of consistent data collation across both Australia and Aotearoa New Zealand in this important part of maternal health leaves both healthcare providers and governments as well as the women and their families at a state and federal level unable to assess the needs for improvement with healthcare systems.
Across both countries, over 25 hospitals are participating in data collection and analysis in preparation for presentation over successive sessions during the ASM: data collection from various sites across both Australia and Aotearoa New Zealand has proved challenging, with participating hospitals citing both the lack of workforce resources in being able to collect this data, along with antiquated systems of data collection and collation as barriers to providing accurate and up-to-date data for analysis.
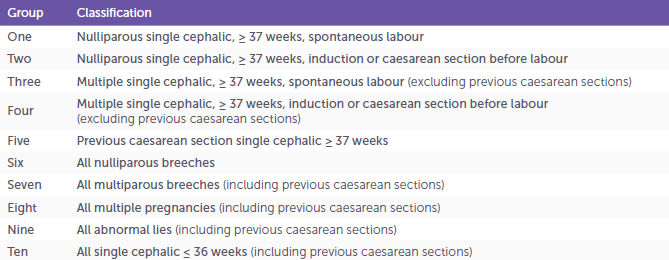
The aim of these sessions is to aggregate information from multiple maternity care providers throughout Australia and Aotearoa New Zealand into a series of presentations of the data gathered. The intention is to showcase the data in a concise manner, followed by a panel discussion, led by Dr Michael Robson, the creator of the Classification System, who will delve into the trends and further discuss the current situation which healthcare systems find themselves, in relation to several factors relating to labour and birth outcomes. TGCS classifies women into the following groups which are totally inclusive and mutually exclusive.6
Using the TGCS, a number of other events and outcomes within the data sets are considered to uncover trends within labour, including: rate of epidurals, rate of obstetric anal sphincter (OASI) injuries, use of Oxytocin, Post Partum Haemorrhage rate (≤1000ml), Spontaneous Vaginal Birth Rate, Operative Vaginal Birth Rate, Caesarean Section Rate, Caesarean Section Rate at full dilatation, Neonatal Unit Admission, Hypoxic-ischemic Encephalopathy Rate and APGAR <7 at 5 minutes.
For improvement of outcomes by practitioners, and to be able to influence policy and improve maternal outcomes and implement better systems for collection and collation of data, it is integral for large-ranging studies to be undertaken by our colleagues. It is hoped that by undertaking this vitally important project, there will be momentum to further improve outcomes for the women in our care with larger scale state, region and national data collection and interpretation.
Other studies using the TGCS overseas shows that the approach to labour outcomes vary greatly based on health systems within a similar geographic region. Important insights into the rate of caesarean sections and trends within Europe between 2015-20197 are shown through an in-depth analysis using Euro-Peristat. The advantage of this study is Euro-Peristat was able to access TGCS data from twenty-seven countries within the European Union, as well as those within the geographical region outside the zone (Norway, Iceland, Switzerland and the United Kingdon), through an established network8 which provided a wide ranging and comprehensive data set for the rate of caesarean sections. The ability to contribute data was shown to be varied throughout the participating countries, as only just over half were able to provide all the data for the TGCS for review.9 It further showed a decreasing rate in a third of countries in their caesarean section rate overall, however countries which were not able to contribute full data from the TGCS, tended to have the highest rates of caesarean section in the cohort.10
In countries with similar populations and healthcare systems, using the TGCS allows for benchmarking between comparable nations. Additionally, it highlights the impact on the health of mothers and babies.11 Since original publication in 2001, the TGCS has been recommended by the World Health Organisation (WHO) for use worldwide to better understand birth rates and outcomes.12 It is hoped that as more countries take up this data classification tool, our understanding of birth outcomes will significantly improve. Data analysed in the Euro-Peristat study in some cases was estimated, calculated and included in final report numbers in cases where the data was not available13, however for hospitals which are participating in the Australian and Aotearoa New Zealand data collection, they are encouraged to include these gaps in their data as part of their submission and presentation to further highlight the data collection issues which healthcare systems in both countries are currently facing.
Further analysis using the TGCS in various settings has provided detailed insights. For instance, a comprehensive study over 11 years at a tertiary teaching hospital in Singapore revealed a significant increase in caesarean sections. This long-term analysis highlighted the need to reduce caesarean rates by promoting vaginal births for nulliparous women and increasing the rate of vaginal births after caesarean section. The findings showed that these two cohorts were the primary contributors to the rising caesarean rates in this locality during the analysed period.14
Analysis of a Swedish maternity unit, which conducted a continuous audit from 2013-2016 of all births in their location to understand quality improvement for women and children, effectively utilised the four years of data collected to revise and improve hospital policies and guidelines, resulting in better maternal outcomes.15 The authors of this study noted that the continuous use of the audit based on “clinically significant classification”16 ensures the ability to improve quality. From the same cohort of patients, a study was conducted to assess their experiences of labour. The results revealed that satisfaction with labour was influenced by several factors, including duration of labour, the use oxytocin, epidurals, and mode of birth data points also collected as part of the TGCS.17
It is hoped that contributing hospitals continue to collect and reflect on their own data and trends, and that this practise will expand to more hospitals within both Australia and Aotearoa New Zealand. This expansion will facilitate data comparisons between Australia and Aotearoa New Zealand and similar international institutions.
This data will be presented at the RANZCOG ASM from 14-16 October 2024, in Wellington, Aotearoa New Zealand. I would like to take this opportunity to thank all hospitals involved for their hard work and contributions, as well as Dr Michael Robson, the Besins Healthcare Keynote Speaker, and Ms Sara MacArthur and Ms Kathleen McKinn from the RANZCOG Events Team who have been integral to the success of this project.
References
- Robson M., Classification of Caesarean Sections, Fetal and Maternal Medicine Review, 2001, pp.23-29
- Amyx, M et al., Trends in caesarean section rates in Europe from 2015 to 2019 using Robson’s Ten Group Classification System: A Euro-Peristat study, 2023, pp.444-454
- Australian Institute of Health and Welfare, National Core Maternity Indicators, July 2023
- New Zealand Maternity Clinical Indicators, 2018, Trends, Te Whatu Ora, 2018
- New Zealand Clinical Indicators Background document, Te Whatu Ora, 2023
- Robson M., Classification of Caesarean Sections, Fetal and Maternal Medicine Review, 2001, pp.23-29
- Amyx, M et al. Trends in Caesarean Section rates in Europe from 2015-2019 using Robson’s Tean Group Classification System: A Euro-Peristat Study, pp.444-454
- Amyx, M et al. Trends in Caesarean Section rates in Europe from 2015-2019 using Robson’s Tean Group Classification System: A Euro-Peristat Study, pp.444-454
- Amyx, M et al. Trends in Caesarean Section rates in Europe from 2015-2019 using Robson’s Tean Group Classification System: A Euro-Peristat Study, pp.444-454
- Amyx, M et al. Trends in Caesarean Section rates in Europe from 2015-2019 using Robson’s Tean Group Classification System: A Euro-Peristat Study, pp.444-454
- Zeital, J et al., Using Robson’s Ten-Group Classification System for Comparing Caesarean Section Rates in Europe: an analysis of routine data from the Euro-Peristat Study, pp.1444-1455
- Robson Classification: Implementation Manual. Geneva: World Health Organisation; 2017.
- Zeital, J et al., Using Robson’s Ten-Group Classification System for Comparing Caesarean Section Rates in Europe: an analysis of routine data from the Euro-Peristat Study, pp.1444-1455
- Chong C et al., Changing Trends of Cesarean Section Births by the Robson Ten Group Classification in a Tertiary Teaching Hospital, 2012, pp.1422-1427
- Kempe P and Vikström-Bolin M, The Continuous Audit of Events and Outcomes of Labour and Birth Using the Ten Group Classification System and its Role in Quality Improvement, 2019, pp181-188
- Kempe P and Vikström-Bolin M, The Continuous Audit of Events and Outcomes of Labour and Birth Using the Ten Group Classification System and its Role in Quality Improvement, 2019, pp181-188
- Kempe P and Vikström-Bolin M, Women’s Satisfaction with the Birthing Process in Relation to Duration of Labour, Obstetric Interventions and Mode of Birth, 2020, pp.156-159


Leave a Reply