

Angiomatosis is a vascular malformation characterised by a diffuse network of variably sized blood vessels involving multiple tissue planes. It is known to affect skin, deep soft tissue, bone and are often clinically extensive. Angiomatosis of the uterus and cervix is extremely rare, with a paucity of literature describing this phenomenon. To our knowledge, only one other case report has described this condition, which was in a 27-year-old female who presented with intractable menorrhagia unresponsive to all conservative forms of treatment.1 We present an unexpected case of angiomatosis of the uterus and cervix in a young female.
A 29-year-old woman presented with a long-standing history of dysmenorrhea and menorrhagia resulting in iron deficiency. She had five uncomplicated vaginal deliveries with no other relevant medical history. A transabdominal and transvaginal ultrasound demonstrated a normal endometrial thickness of 4.4mm, no focal lesions and a homogenous myometrium. The initial clinical impression for her symptoms was adenomyosis. A trial of a hormone-releasing intrauterine device was poorly tolerated as it worsened her symptoms. She declined other conservative measures and opted for an elective total hysterectomy for definitive treatment.
Macroscopically, the uterus appeared symmetrical and mildly enlarged with a dusky appearance. Sectioning showed a band-like dark purple discoloration of the outer one third of the cervix and myometrium associated with prominent blood vessels (Figure 1). Histological examination featured angiomatosis, characterised by a diffuse permeation of the outer half of the myometrium and cervix by a mixture of thick- and thin-walled vascular channels of varying sizes, lined by flattened, benign endothelial cells (Figure 2). The endometrium showed early secretory changes with no other abnormalities to account for abnormal bleeding. The fallopian tubes, which were also removed, did not demonstrate angiomatous lesions. She recovered well from the surgery.
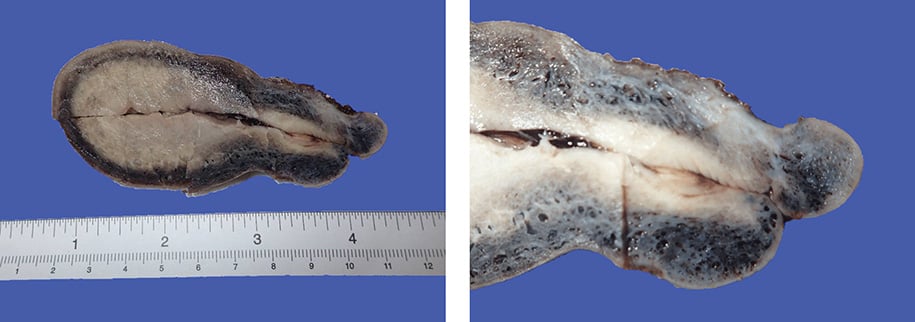
Figure 1. (Right) The uterus shows a continuous peripheral rim of dark purple discoloration. (Left) The area of discoloration appears to be representing numerous congested blood vessels.
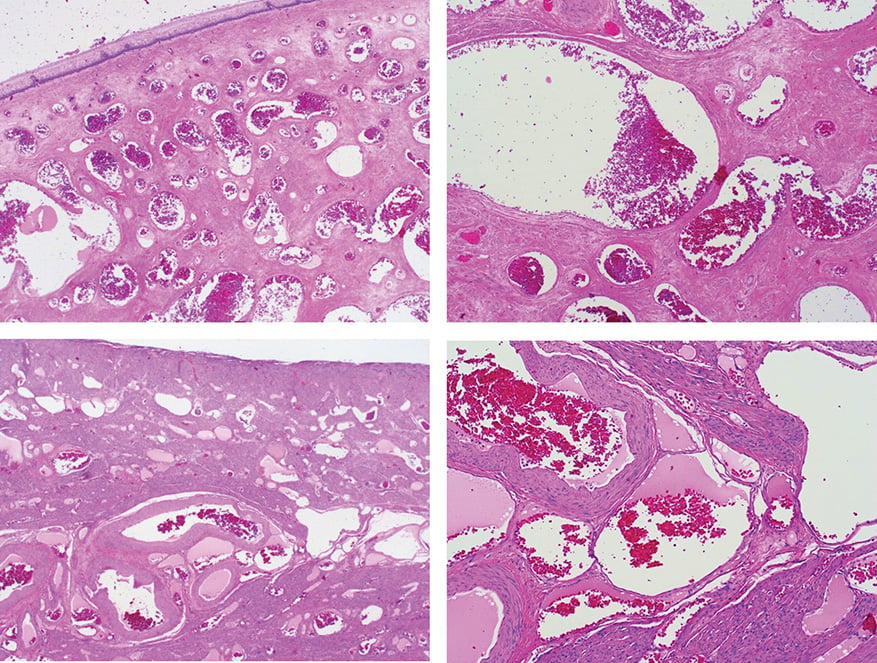
Figure 2. (Top right and left, H&E) Uterine cervix show numerous ectatic vascular channels lined by benign endothelial cells. (Bottom right and left, H&E) Uterine corpus similarly show vascular channels of varying sizes extensively involving the myometrium.
Angiomatosis, which is regarded as a diffuse form of hemangioma, is not included in the standardised nomenclature as a disease of the uterus and cervix. As a result, this condition is likely to be underdiagnosed and it continues to represent a pathological curiosity. Moreover, clinical examination and routine investigations for menorrhagia, including hysteroscopy, endometrial curettage and ultrasonography, are likely to be unhelpful in this instance. Therefore, definitive diagnosis of angiomatosis relies heavily on histopathology.
Angiomatosis in the usual deep soft tissue sites can cause pain and persistent swelling that is worsened with strenuous exercise. Moreover, conventional angiomatosis can be associated with certain syndromes such as Klippel Trenaunay syndrome, Sneddons syndrome or Gorham disease.2 However, the clinical presentation and significance of this histological finding in the uterus and cervix is largely unknown. In a similar case report of a 27-year-old with angiomatosis of the uterus, cervix and fallopian tubes by C Pontre et al,3 the patient presented with intractable heavy menstrual bleeding that is unresponsive to all conventional and conservative forms of treatment. On a slightly different note, within the same spectrum of vascular lesions, a retrospective study conducted in Taiwan on uterine haemangiomas, it was found that one of the most common presentations is menorrhagia.4 Likewise, heavy, painful menstrual bleeding represents the chief complaint of our index case. Therefore, it appears that angiomatosis of the uterus and cervix represents a feasible explanation for heavy menstrual bleeding in young females with no other identifiable cause. This is especially true in patients who are not responding to standard treatments.
As histopathological examination is the key to definitive diagnosis of angiomatosis of the uterus and cervix, maintaining a broad differential diagnosis and having a good understanding of various benign vascular lesions of the uterus and cervix is of paramount importance. More research into understanding the pathogenesis of this condition in the uterus and cervix will be the next step going forward. This should be followed by the development of diagnostic criteria and management guidelines to prevent undertreatment and/or overtreatment.
References
- Pontre JC, Ojedo V, McElhinney B. Angiomatosis of the uterus, cervix and fallopian tubes: a rare and benign cause of intractable, heavy menstrual bleeding. BMJ Case Rep. 2017;2017:bcr2017221975.
- Khan S, Pujani M, Jetley S, et.al. Angiomatosis: A Rare Vascular Proliferation of Head and Neck Region. Journal of Cutaneous and Aesthetic Surgery. 2015;8(2):108-10.
- Pontre JC, Ojedo V, McElhinney B. Angiomatosis of the uterus, cervix and fallopian tubes: a rare and benign cause of intractable, heavy menstrual bleeding. BMJ Case Rep. 2017;2017:bcr2017221975.
- Chou WY, Chang HW. Uterine Hemangioma: A Rare Pathologic Entity. Arch Pathol Lab Med. 2012;136(5): 567-71.

Leave a Reply